- RN Forward
- Posts
- 🗞️ Autonomous Prescriptions, Corporate Lawsuits, and the AI Healthcare Arms Race
🗞️ Autonomous Prescriptions, Corporate Lawsuits, and the AI Healthcare Arms Race
OpenAI and Anthropic launch competing healthcare AI products, Utah pilots autonomous prescription renewals, and Epic sues over alleged patient data fraud.
Niki Pham
January 16, 2026

Team Huddle
Hi, its me. Your absentee Nurse, back from from the depths of the infamous supply room where you literally can’t find anything and realize months have gone by when you do leave. So much so that its a whole new year. 😅
2026 kicked off with a doozy of announcements which we’ll go over briefly today. OpenAI + Anthropic move publicly into the healthcare space, Doctronic is first to abandon the “clinician in the loop” trope, Epic goes on the offensive (aka. lawsuits), and more.
But before we get into it, ya girl’s trying to find more nurse founded companies that scale. Here are the requirements i’m looking for. Do you know any companies that fit this criteria? Please email me (i’m desperate)!

News Nurses Need to Know
OpenAI + Anthropic enter the healthcare market but in significantly different ways.
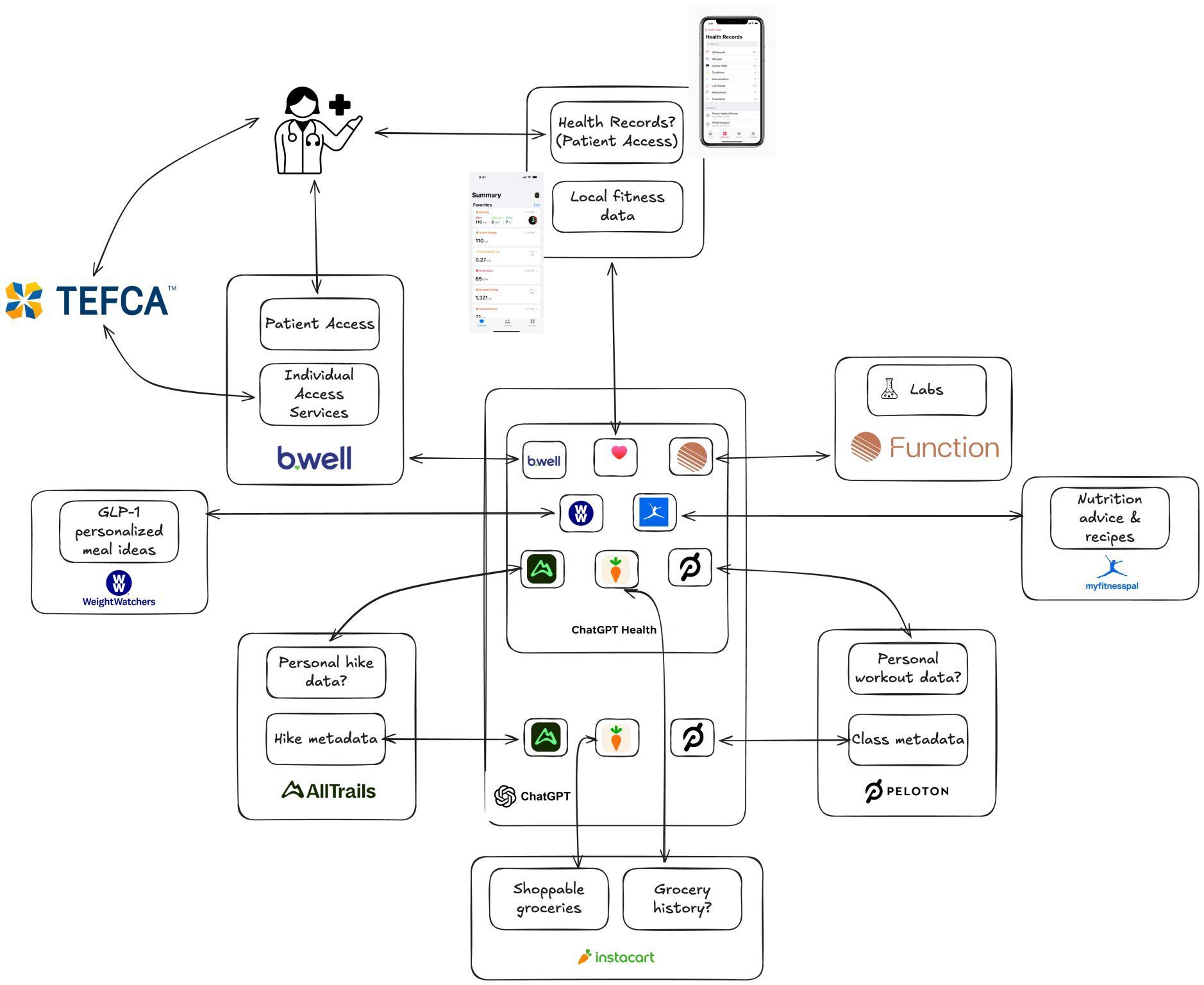
Details: Ahead of JPM26, OpenAI and Anthropic both launches healthcare AI products within one week from each other. OpenAI launched two products: ChatGPT Health (consumer-focused) and OpenAI for Healthcare (enterprise). They emphasized personal health record integration through b.well, Apple Health, and wellness apps (ie. MyFitnessPal, etc).
Their consumer pitch: Help people understand diagnostic results, prepare for appointments, and manage their health data in a HIPAA-protected space. Evidently, 230 million people ask health related questions already anyway. 🤷🏻♀️ Their enterprise pitch: Have hospitals like UCSF, MSK, and Cedars-Sinai use GPT-5 for clinical decision support (CDS) and workflow templates. An in-house GPT wrapper for healthcare if you will.
Anthropic positioned Claude for Healthcare almost oppositely. They’re going all in on enterprise infrastructure. Their announcement featured collaboration with Banner Health and emphasized tools for pharma, payers, and health systems (Connected to CMS coverage databases, ICD-10 coding, National Provider Identifier Registry, Medidata clinical trials platform, and ClinicalTrials.gov). Basically all the unsexy stuff that makes people money in healthcare. And by money, i’m talking millions annually. As Rik Renard points out, one enterprise deal closed by Chai Discovery (backed by OpenAI) with Eli Lilly will generate mid-eight-figure annually which dwarfs in consumer subscription revenue (i.e. hypothetical $20/month/per person). 🤑 Consumer health record integration was more of a secondary positioning for them.Why it matters: OpenAI and Anthropic are coming for CDS tools like OpenEvidence + consumer targeted EHR management companies (like nurse-founded company Primary Record). If you’re building AI CDS tools or consumer facing apps that assist with EHR management or care navigation/advocacy, choose a vertical and build deep into it. A good example of this is nurse-founded company, Family Room. They help families with loved ones in the ICU. While the product is still early, if they build it out to include AI (personalized analytics, interdisciplinary round notetaker, personalized guided meditation/prayers, etc.) they can OWN the entire family (“consumer”) experience of being in the ICU from start to finish. Thats a defensible moat worth building.
Both companies extensively consulted physicians in validating the model, but as always, there is minimal nursing visibility in product development. To be fair, these tools embed into Medicare coding, clinical trial protocols, and hospital revenue cycle operations. But i’d argue that nurses end up executing some of these workflows (i.e. clinical research nurses) risk becoming end-users designed without our operational expertise, therefore repeating the EHR implementation mistakes of the past decade. As the product development grows, we’ll see how they build for nursing and other allied health professionals.
Doctronic and the State of Utah (Yes, of ”Secret Lives of Mormon Wives” notoriety Utah) partnered to pilot autonomous prescription renewals.
Details: Utah launched a 1st ever (in the US at least) pilot program allowing Doctronic’s AI system to autonomously renew prescriptions for chronic conditions with no human physician involves. It can refill 190 commonly prescribed medications (excluding controlled substances like pain meds, ADHD drugs, and injectables). Patients just visit a webpage, verify UTah residency, and the AI pulls prescription history, asks clinical screening Qs a physicial would typically ask, and sends the approved renewal directly to pharmacies for $4/prescription. Utah cites cost reduction, medication lapse prevention, easing provider shortages, and supporting innovation pathways as reasons for their venture. Doctronic’s CEO Dr. Adam Oskowitx states “The Ai matched physician treatment plans 99.2% of the time across 500 urgent care cases”. They secured bespoke malpractice insurance covering the AI system itself. They plan to expand to TX, AZ, and MO.
Why it matters: IMO, its giving standing orders which nurses utilize all the time. In this case, its automating standing orders using “if/then” logic. Refills are a great place to start. I’m not convinced of creep into nursing scope of practice as i’m hard pressed to find any APP who enjoys monotonously refilling prescriptions of patients who’ve been on Lipitor for 20+ years with no issues. 😅
Its also matters because this is the first time physicians are not held liable for mistakes of a startup’s AI. I would give my left pinkie toe nail to see the underwriting for their malpractice insurance. The FDA declined to comment saying it falls outside of their purview even though Doctronic’s product is giving Medical Devices. Which leads to our next topic re: FDA ….
The FDA Exemptions Digital Health Companies Are Using to Skip Clearance in 2026 (Parts I and II) by Elevare Law
Details: Building on the 21st Century Cures Act, the FDA released guidance expanding regulatory exemptions for General Wellness Products and CDS software. The result = healthtech companies can market a lot more without FDA clearance. Products using non-invasive sensing to estimate physiologic parameters like BP, SpO2, blood sugar, and heart rate variability are allowed as long as they’re not “diagnosing or treating”.
For CDS tools, the FDA expands what AI-enabled clinical tools can do without FDA clearance. They now allow software companies that provide clinical recommendations to clinicians to qualify as “non-device CDS” as long as it meets there 4 criteria: 1) not intended to process medical images or signals/patterns from diagnostic divides, 2) displays/analyzes “medical information” (patient data communicated between clinicians, supported by peer-reviewed sources), 3) provides recommendations to healthcare professionals for prevention, diagnosis, or treatment (not patients directly), and 4) enables independent review of the recommendation basis so clinicians don’t “reply primarily” on the software. think transparency of data sources, methods, models, adn techniques.Why it matters: Re: wellness products, there will be a grey market of quasi-clinical tools that patients trust as medical-grade. Expect to translate metrics from “wellness devices” taking into account nuanced scenarios (like how SpO2 readings during exercise differs from diagnostic pulse ox readings).
Re: CDS tools, there are products being made for us as we speak. Heck, my hackathon team mates and I built a Code Blue one last may in 2 days. With loose regulation from the FDA, expect more CDS tools with nurses as end users. Think active labor CDS, bedside intubation CDS, etc. The possibilities are endless however we must hold these tools accountable by validating their outputs.
Epic lawyers up and sues over data fraud.
Details: U.S.’ largest EHR company, Epic, filed a federal lawsuit against Health Gorilla, Critical Care Nurse Consultants + other telehealth companies for fraudulently accessing patient data. They argue that these companies “masqueraded as healthcare providers” to access patient data for litigation and monetization purposes rather than treatment. A key example: Mammoth Rx (cofounded by Daniel Baker) allegedly pulled 13k+ medical records from Epic customers including Trinity Health and OCHIN members starting Oct. 2024. When Mammoth sent data beck to patients’ doctors, it was lists of test without results, suggesting no actual treatment occurred. The lawsuit also connects Mammoth Rx CEO Ryan Hilton to Nationwide Healthcare Provider Corp, which markets records to attorneys.
Joining Epic in the lawsuit is Oregon Community Health Information Network (OCHIN), Reid Health, Trinity Health, and UMass Memorial Health.Why it matters: Patient data protection is on everyones mind (I mean just look at all the talk around consent, HIPAA, and patient’s uploading their medical records to GPT Health above). Sen. Ron Wyden (D-Ore.) just asked EHR companies to implement tools to give patients greater control over data access while Sen. Bill Cassidy (R-La.) introduced legislation to protect health data from wearables and apps not covered by existing federal privacy laws.
Moreover, Critical Care Nurse Consultants (doing business as GuardDog Telehealth) is named among the defendants insinuating that a nurse-owned company potentially participated in fraudulent behavior and/or they used the nurse credentials to access data.
A few bigger picture questions posed from this lawsuit are:
1) Are bad actors exploiting the trust-based interoperability model by parading as “treatment” providers to get access to patient records then in turn, monetizing them? Or is Epic using “patient privacy concerns as a cover for anti-competitive behavior/controlling who gets access to health data to maintain market dominance?
2) Who is responsible for policing data access?
3) How do we maximize legitimate data sharing for better patient care while preventing fraudulent access?
4) Why are there no mechanisms for patients to determine who gets access to their records?
Offcall’s 2025 Physicians AI report
Details: Physicians are adopting AI on their own, often using personal subscriptions to tools like OpenEvidence because their orgs are not moving fast enough (81% are dissatisfied with their employer’s AI adoption speed). Overwhelmingly, doctors agree that AI makes them better at their job with 67% of them using AI in their daily practice. However, 71% have little to no influence on which AI tools get used and 48% say employer communication about AI is poor.
Why it matters: Yes, this is a newsletter about nurses so why am I including a physician report? Well, because Nurses are the next end-user healthtech companies are starting to build for (i.e. Abridge ambient scribing, Voize companion for nurses, nurse-founded Adni’s AI agent Allie, etc). We can infer a lot from our physician colleagues sentiments. With the slow pace of health systems adopting and implementing new AI tools, I predict that speed of rolls outs won’t change in the next year. I would go as far to say that nurse will feel like they have even less influence on which AI tools get used than physicians. The fact is, nurses are not invited nor present in regular conversations that affect our workflows, so what difference with it be for AI implementation?
Alas, this defeatist attitude is not what i’ll leave you with. I encourage every nurse reading to be THAT nosy Nancy, and start asking questions. JOIN your governance committee, ATTEND that town hall with the hospital CEO, PARTICIPATE in your union activities. Healthcare is at an inflection point and we will be RNing towards it. 🏃🏻♀️

Funding Announcements
💸 = Hiring potential. Follow these companies closely to see Nurse-qualified positions posted. Remember: Just because some positions don’t say “Nurse”, doesn’t mean you aren’t qualified!
Pomelo Care, a virtual maternity care model, raised a $92M Series C. at a valuation of $1.7B.
Safety platform for health systems, Canopy, raised $22M. (Disclaimer: I am apart of the Scrub Collective within Scrub Capital who invested in this round.)
Oasys Health, the AI OS for behavioral health clinics raised $4.6M.
Other Notable HealthTech Reads, Podcasts, and Vids
READ
📚 Policy brief: ambient AI scribes and the coding arms race in NPJ’s Digital Medicine
📚 Ambient AI Scribes—What Is the Return on Investment? in JAMA
📚 The Clinician’s Guide to Breaking into Digital Health by fellow clinician Carly Newhouse
📚 State of Clinical AI Report 2026
📚 Hospitals are a proving ground for what AI can do, and what it can’t by the WSJ
LISTEN
🎧 Why securing AI is harder than anyone expected and guardrails are failing | HackAPrompt CEO in Lenny’s Podcast
🎧 Klorporate Espionage series by Kayla Basset where she interviews clinicians who have transitioned into non-traditional roles (think Founders, Product Managers, Operators, and more!)
WATCH
📺 OpenEvidence Valuation, New LLM Study, CMS new ACCESS Model, EO on AI with Rik Renard RN, Sergei Polevikov, and Alex Koshykov. 2025 Healthcare in review and some 2026 market predictions from experts!
📺 AI Prescription Medication Renewals Discussion with Doctronic’s Co-Founder Dr. Adam Oskowitz with Health Tech Nerd’s Kevin O’Leary
On The Blog ✍️

Forward Nursing: Innovation Opportunities 🏃🏻♀️
Round-up of career and business development opportunities i’ve come across that can help nurse innovators like YOU! (Not sponsored or affiliated with RN Forward.)
Nursing Innovation Fellowship Program 2026-2027 from UPenn SON + Wharton School
TBH: Learn human centered design and design thinking methodologies while upskilling on your bizznezz acument through Wharton’s Executive Education cirriculum.
Where: Remote
Cost: Free thanks to Johnson & Johnson sponsorship
Eligibility: Chief Nursing officer (CNOs), Nurse executives, and senior nurse leaders (charge nursing counts IMO!)
Due Date: February 10, 2026
Apply here
25m Health’s AI Prototyping Workshop
TBH: Who needs a CTO to build a prototype anymore? Not you after taking this ✨vibe coding✨ workshop. Anyone can take this class!
Where: Remote
Cost: Free
Due Date: February 10, 2026
Sign up here
Reply