- RN Forward
- Posts
- 🗞️ ChatGPT for Clinicians, a GLP-1 Scam, and the Nurse-Founded Research I've Been Laboring On
🗞️ ChatGPT for Clinicians, a GLP-1 Scam, and the Nurse-Founded Research I've Been Laboring On
OpenAI launches ChatGPT for Clinicians, the NYT profiles an "AI company" that turned out to be a GLP-1 scam, and I'm finally sharing what I've been researching about nurse-founded companies that scale.
Niki Pham
May 01, 2026
Team Huddle
After months of research paper writing hell, I am back back back back again (IYKYK). Who thought it’d be a good idea to let me write a paper? Who knows. But I was definitely today years old when I found out that you don’t need to be associated with a University or have a PhD to do “research”. However, it does help to have mentors who have background in academic rigor to guide you along the process (cue FINE Fellowship plug here). So if a rando nurse like me can do it, so can you! Just find a niche you’re curious about, start asking questions, and formalize those solutions. Odds are, other nurses have been asking the same questions too.
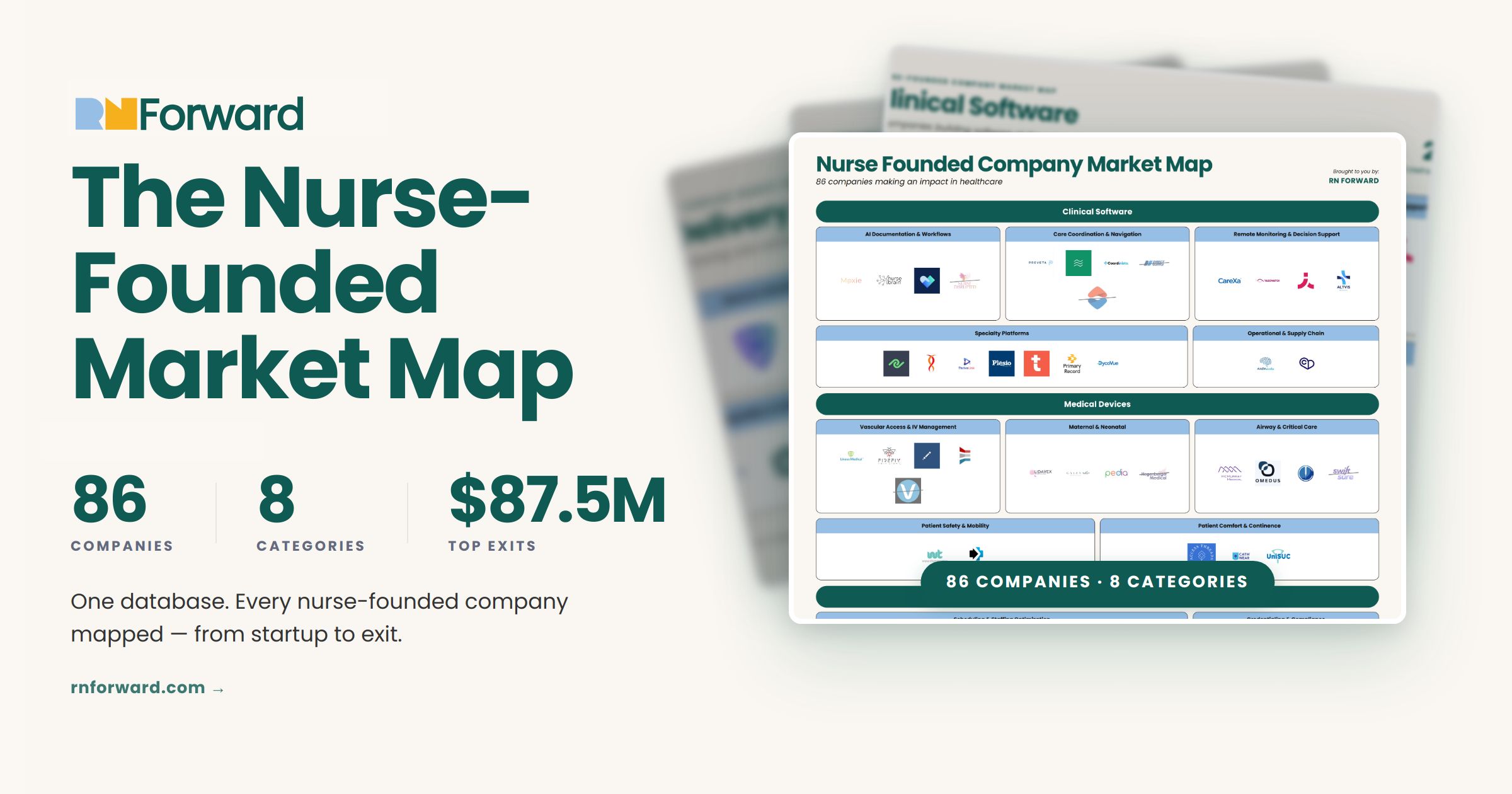
For me, the questions that plagued my mind were: Which types of nurse-founded companies scale, and how are they funded? Which business categories attract institutional capital and which do not? Which funding sources are used to working with nurse-led ventures? What network of nurse entrepreneurs can a new nurse entrepreneur go to for advice?
So I whittled down my paper to focus on 2 objectives:
Objective 1: Identify the business models, funding patterns, and operational characteristics of nurse-founded companies that have achieved significant scale (successful acquisition, 51+ employees, or $1M+ in funding).
Objective 2: Analyze funding trajectories and outcomes across 8 business categories to determine which models attract capital and demonstrate economic viability.
I am hoping to get an abstract out into the world by Fall 2026 but that doesn’t mean I can’t share the results with the RN Forward ride or dies first. Subscribe, tell your nursing friends, and stay tuned. Because it’s coming. 😉
News Nurses Need to Know
AI Nurse Specialists: Transforming the nursing workforce for the age of artificial intelligence
THE DEETS: The authors proposed that nursing roles in AI implementation is limited to bridging the gap between AI tools and bedside nurses who lack formal AI training, translating nursing workflows into AI models, collaborating with engineers, and ensuring tools align with nursing practice. Sounds good but is actually not good enough.
The problem with this set up is that it positions nurses as retrofitters of poorly-designed tools rather than demanding seats at the tables where OpenAI, Epic, and other health tech companies actually build AI products. The job description ("liaise with vendors," "validate AI outputs," "help technical teams understand nursing") is damage control language. It's the EHR implementation story all over again: technologists build systems, nurses clean up the mess because there was no nursing representation at the start of the build.WHY IT MATTERS: Until nurses sit on AI company boards, chair hospital AI purchase committees, and hold veto power over workflow specialist roles just add another layer of nursing labor compensating for everyone else’s failure to include us from the start. Their proposed solutions (that we agree on!) are:
✅ Nurses at the cap table when AI companies raise funding
✅ Nurses deciding which tools get hospital contracts
✅ Nurses with authority to say "no" when products don't meet workflow needs
Elion Health’s Clinician Recruiting Mapping Markets: The technology tackling hiring timelines briefing.
THE DEETS: Post-pandemic, CFOs took control of staffing decisions after travel nurse rates hit $200-250/hour, often preferring vacancies over contingent labor costs, making permanent hiring pipelines the highest-return option despite how inefficient it is.
The clinician recruiting technology market splits along physician versus nursing workflows. Nurse recruiting automates via AI voice screening, SMS outreach, and mobile-first applications. In this situation, speed wins because credential sets are standardized and volume is high. Physician recruiting requires "ego-aware" relationship management with months-long timelines. Advanced practice providers (NPs/PAs) increasingly fill physician gaps in primary care, creating a middle tier between these models.
The vendor landscape includes: 1) Physician sourcing databases (Doximity Talent Finder, PracticeMatch, PracticeLink, DocCafe) maintaining proprietary clinician networks. I would argue Adni can fit here but for nurses. 2) Healthcare-specific ATS platforms (symplr Recruiting, Marketware, Hireology, Apploi, Intelliworx, Syncx) embedding specialty taxonomy, state licensure tracking, and credentialing integration that general platforms (Workday, iCIMS, Oracle) require months to customize. 3) Permanent clinician marketplaces (Incredible Health, Aya Healthcare's CoreHire, Hallmark Health Care Solutions) collapsing sourcing and screening into single-step delivery of pre-vetted interested candidates, competing with agencies on speed for permanent roles.
WHY IT MATTERS: I consider this the most up to date market update on staffing and recruiting in healthcare thats not a bajillion pages to read (only caveat is that its not totally nursing specific).
Nursing Workforce is one of the problems that many nurses aim to solve as founders and operators. For example, Tallewise (formerly Goodwork) and Nurse Connect are newer nurse founded startups hoping to disrupt the space while well funded late stage nurse founded startups like Intelycare and Connect RN (who have raised $270.8M combined) have achieved scale and established health system partnerships. This doesn’t even include non-nurse founded company competition like Aya Health or Incredible Health. If you are building in RecruitingTech, prepare yourself for entering a complex and crowded market. This article will tell you the general lay of the land.
For bedside nurses, this article supports we’ve always known: CFOs control staffing decisions and they’re choosing vacancies over travel nurses. This means understaffing becomes a deliberate financial strategy rather than a crisis to solve. Anticipate baring the patient safety consequences of short-staffing while health systems work to avoid agency premiums.
OpenAI's ChatGPT for Clinicians — the latest move in a three-product healthcare stack built in four months.
THE DEETS: On April 22, 2026, OpenAI launched ChatGPT for Clinicians — free, verified access (NPI required) for U.S. physicians, NPs, PAs, and pharmacists. It sits between their consumer product (ChatGPT Health) and their enterprise product (ChatGPT for Healthcare, already deployed at HCA, Cedars-Sinai, Boston Children's, and others). Features include GPT-5.4, cited clinical search, reusable workflow skills for prior auth, referral letters, and patient instructions, deep literature research, and CME credits. HIPAA support via BAA is available but opt-in (not the default. Conversations are not used to train models. The direct competitor this targets is Open Evidence (currently the largest clinician-facing AI platform globally, with ~15M consultations/month from 757K+ verified clinicians), a $12B valuation, and embedded into Mount Sinai's Epic EHR as of March 2026. Open Evidence is also free (but funded by pharma ads during loading screens). OpenAI's model is different: the free individual tool is likely a funnel to sell enterprise contracts to those same clinicians' hospital systems.
Clinicians who ran head-to-head comparisons found ChatGPT for Clinicians to be the weakest of the three main tools on raw clinical answer quality — behind Doximity GPT on citation precision and Open Evidence on speed and research depth. OpenAI's own consumer-facing ChatGPT Health was also independently found to under-triage and over-triage emergencies in a Mount Sinai Nature Medicine study. This is a meaningful gap from their internal benchmarks.WHY IT MATTERS: This is a very hot space right now, and this launch is a signal of just how fast it's moving. For NPs specifically, free access to clinical-grade AI changes the math — most of these tools have historically lived behind expensive enterprise contracts that left independent practices on the outside. But "free" is worth scrutinizing. Open Evidence is free because pharma is paying to serve you ads at your clinical decision moment (CPMs/Cost per 1k ad impressions reportedly in the $70–150+ range.) That's a monetization model worth being aware of: the ad-funded model raises real questions about whether commercial interests can creep into what gets surfaced and how. OpenAI's funnel model is more transparent but has its own agenda. Use these tools, but understand who benefits when you do.
The New York Times profiled an "AI company" and missed basically flopped hard on it. (Here's the original NYT piece, and here's Futurism's more complete version of events.)
THE DEETS: On April 2, 2026, the Times ran a glowing profile of Medvi, a GLP-1 telehealth startup run by two brothers. The pitch: AI enabled a solo founder to build a business projecting $1.8B in 2026 sales. OpenAI's Sam Altman said he'd "like to meet the guy." The piece went viral. What the Times left out: the FDA had sent Medvi a warning letter on February 20 for misbranding compounded semaglutide and tirzepatide. A class action lawsuit had been filed 13 days before publication for deceptive spam. Futurism had documented AI-generated patient photos, fabricated doctor personas, and physicians whose names appeared on the site without their knowledge. Big yikes. Medvi's clinical infrastructure partner OpenLoop also suffered a 1.6 million-record data breach in January 2026, and a separate lawsuit alleges their compounded oral tirzepatide has no viable absorption pathway. After reader backlash, the Times updated the article, writing: "Our piece should have included that information." Medvi blamed rogue affiliates.
WHY IT MATTERS: NPs are actively being recruited by GLP-1 telehealth companies to serve as the prescribing provider on their platform. Your license is what makes the whole operation legal. Compliance failures, outsourced clinical operations, and a data breach at the infrastructure partner should be sussed out during your interview and get your spidey senses tingling. Before signing on with any telehealth company, look hard at how they actually operate. The broader issue here is that this story is really about what happens when AI becomes a marketing engine, not a care delivery tool. Medvi is not an AI healthcare company. It is a distribution funnel for compounded drugs, dressed up with GPT-generated copy, AI stock photos, and fake before-and-afters. The fact that the Times initially presented it as the future of medicine says something about how easy it is to launder a healthcare scam through AI hype. For nurses building in this space or evaluating vendors: AI does not change the liability question. Someone is still responsible for what gets prescribed and what happens to the patient after. & its probably you.

Funding Announcements
💸 = Hiring potential. Follow these companies closely to see Nurse-qualified positions posted. Remember: Just because some positions don’t say “Nurse”, doesn’t mean you aren’t qualified!
Courier Health, a company that helps pharma companies manage patient experiences, raised $50 million. Oak HC/FT led the round.
Tava Health, a behavioral health platform, raised $40 million. Centana Growth Partners led the round.
Zócalo Health, a community health worker model for Hispanic populations, raised $15 million.
Almanac Health, an AI platform for clinical decision support, raised $10 million. F-Prime led the round.
Keebler Health, an AI platform using clinical data for risk adjustment, raised $16 million. Flare Capital Partners led the round.
Wavelet Medical, a fetal EEG monitoring system, raised $7 million.
AI clinical assistant vendor Thesis Care (formerly Trovo Health) raised a $45M Series A and rebranded.
Doctronic, the AI system authorized to refill prescriptions, raised a $40 million Series B.
Clasp, a startup that helps employers retain clinical hires via loan repayment programs, raised $20 million. Crosslink Capital and Digitalis Ventures led the round.
Prax Health, a business-in-a-box model for NP-led clinics, announced $10 million in funding across two rounds. (They've helped 200+ NPs launch their own independent practices so far!)
Dimer Health, a post-acute transitional care service, raised a $13.5M Series A.
Nadia Care, a maternal care model (formerly Cayaba Care), raised $12 million.
AI clinical decision support platform Avo raised a $10M Series A.
Patient monitoring and decision support company Ambient Clinical Analytics raised a $5M strategic investment.
Other Notable Reads and Podcasts
READ
📚 Break Stuff: Ten Things the Healthcare Market Is Telling Us in 2026 by Health Enterprise Partners
📚 The Future of Quality in Medicare and Medicaid: Themes from the CMS Quality Conference by Avalere Health
📚 60+ Digital Health Investors by Massively Better Healthcare
LISTEN
🎧 Laura Demuth MSN NP | Employee #12 to $200M: Building from the Inside on Klorporate Espionage
🎧 An AI state of the union: We’ve passed the inflection point & dark factories are coming on Lenny’s Podcast ✨(MY TOP REC FOR THE MONTH FR FR)✨
On The Blog ✍️

A 👏🏻 Nurse 👏🏻 did 👏🏻 THAT!

Courtesy of Camelback Ventures.
Kwamane Liddell of Thrivelink sat on a panel during SXSW 2026 with Founder, Investor, and tennis legend Serena Williams. He spoke of how he took a problem he saw as a nurse, found a solution, and turned it into a scalable solution with the help of his network.
Thrivelink builds telephonic and digital AI agents (backed by human support) that help families enroll in programs and access the resources they need over the phone, online, or in-person. They do this by partnering with health plans, health systems, and governments throughout the United States.
Forward Nursing: Innovation Opportunities 🏃🏻♀️
Round-up of grants and career development opportunities i’ve come across that can help nurse innovators like YOU! (Not sponsored or affiliated with RN Forward.)
Choosing the Right AI Tools As a Clinician — Offcall AI Residency Webinar Series #2
TBH: Session 2 of Offcall's AI Residency series. Live demo comparing how different AI tools handle the same case, a framework for evaluating any AI tool, and guidance on building a personalized AI toolkit for actual clinical use. Featuring Dr. Michael Hobbs (AI educator + direct primary care pediatrician) and Offcall co-founder Dr. Graham Walker. I hear good things!
When: Wed, May 6, 2026 at 5:00 PM PT / 8:00 PM ET
Where: Remote
Cost: Free
Register here
a16z Speedrun — Startup Accelerator Program (Cohort SR007)
TBH: a16z's early-stage accelerator invests up to $1M in new startups, plus $5M+ in credits from 250+ tool partners. The Summer/Fall cohort includes hands-on operator support across talent, GTM, marketing, recruiting, and visa assistance. Open to founders worldwide.
When: Cohort runs July 27 – October 11, 2026
Cost: Free (equity-based investment program)
Due Date: May 17, 2026 at 11:59 PM PT
Apply here
Fellowship in Nursing Economics (FINE) — Commission for Nurse Reimbursement, Cohort 2
TBH: A 12-month fellowship teaching nurse leaders to speak the language of healthcare finance (reimbursement, payment reform, and system-level decision-making). Includes expert mentorship, policy-relevant capstone project, and a national network of nursing economics leaders. Limited $1,000 Mission Advancement Scholarships available (most applicants who request support receive it, per CNR). I highly recommend this program for anyone who wants to further their career outside the limitations of nursing administration. The connections I made and lessons I learned have been very valuable! (Disclaimer: I was apart of the 1st cohort)
When: Fellowship begins September 2026
Cost: $2,500 tuition; $75 non-refundable application fee
Eligibility: Nurses and healthcare leaders with at least 2 years of professional experience in nursing, healthcare leadership, administration, finance, or operations
Due Date: June 1, 2026
Apply here
Reply